What colour do you associate with the letter “E”? What sound do you hear when you feel the fluffiness of cotton? These sound strange to most people as we experience the senses in distinct ways. However, for 4% of the population, this is a completely normal experience.
Synaesthesia (“joined sensation”) is the neurological phenomenon where two or more senses are coupled together. This creates two kinds of synaesthesia: projection, where you physically sense something (such as seeing a purple circle when hearing piano music), and association, where you associate the sense with another sense (“that sounds quite orange”).
The most common form of synaesthesia that is reported is grapheme-colour synaesthesia, where certain people perceive letters and numbers as different colours. However, there are various kinds of synaesthesia, such as chromesthesia, where people associate sounds with colours (previously called “coloured hearing”). In fact, almost every combination of senses have been described, with some individuals experiencing multiple senses at the same time.
The exact origin and mechanism of synaesthesia are yet to be fully explained. The most likely explanation is that in the brain of synaesthetes, the neural pathways for the various senses cross-over more than they should, causing the simultaneous activation. There are already some cross-overs between these pathways, as evidenced by various sensory illusions that the average person can enjoy. For example, a ventriloquist can fool the audience into thinking the puppet is talking as we hear speech and see the puppet’s mouth moving.
An alternative explanation is that there may be an element of ideasthesia – where concepts are paired with sensory experience. This would mean that synaesthetes are experiencing sensations due to the idea something represents, not because of the original sensory stimulus.
For example, when a synaesthete describes that the word “tree” tastes like brie cheese, it might not be the sound of the word, but rather the concept of a tree that triggers the sensation. We actually see examples of this in day to day life in the form of metaphors. We describe a wine having a round taste or a person being sweet.
There is much to learn about the phenomenon, but synaesthesia has already deepened our understanding of how we perceive the world, process it and commit it to memory through the use of associations and mnemonics.
(NB: I have written MANY ARK posts about the brain and all the delightful ways it screws up. Some of them are probably the most interesting posts on my blog. Please click the hyperlinks to check out the various related articles! 😀 Alternatively, here’s a convenient list: https://jineralknowledge.com/tag/brain/?order=asc)
Among the many organs of the human body, no organ comes close to the magnificent complexity that is the brain. The brain acts as the command centre of the body. It receives massive amounts of information through the various senses, processes it and sends out electrical signals to control how the body operates. Not only does it control “basic” functions such as movement of muscles, controlling organ functions and regulating homeostasis, it is also responsible for the so-called “higher functions” such as consciousness, emotions and cognition. It is the true seat of the mind and soul.
The brain is the only major visceral organ not located in the trunk (body). It is enclosed in the cranium of the skull, which acts as a protective casing. Because it is a closed box, even a small increase in volume (such as due to a bleed or a tumour) can cause extreme pressures to build, causing severe problems. The entire brain and spinal cord are bathed in a fluid called cerebrospinal fluid (CSF), all enclosed by a sheath made of three layers (dura, arachnoid and pia maters). The brain sends out nerves to the rest of the body, which act as electrical wiring transmitting signals. These include the cranial nerves and the spinal cord, which leaves the bottom of the skull down the spine. The spinal cord branches off into many nerves that supply every nook and cranny of the body. The brain itself is made up of two large hemispheres, which are connected by a bridge called the corpus callosum. Despite popular belief, the actions of the two hemispheres are much more complicated than “analytical vs. creative”. The brain also encompasses the cerebellum (the small stripey structure at the back), which controls coordination and speech articulation, and the brainstem, which is involved in autonomic control of life-sustaining functions such as breathing, and also the source of the cranial nerves.
In the last century, scientists have learned that specific parts of the brain play a specific role. This thought started with the field of phrenology, where small areas of the brain were mapped to a certain mental faculty, such as love, wit or destructiveness. Although this turned out to be complete hokum, the idea stayed and we now know the actual functions of each part of the brain. The brain is broadly divided into four lobes: frontal, parietal, temporal and occipital. The frontal lobe is the domain of thought, personality, motor function and other higher functions. The parietal lobe is related to spatial awareness and sensory functions (such as touch). The temporal lobe is linked to hearing, comprehension of language and storing new memories. The occipital lobe is primarily associated with vision. The brain can then be subdivided into more focussed areas, such as Broca’s area that governs speech and Wernicke’s area that governs listening. It should be noted that the four lobes only describe areas on the surface of the brain (cerebral cortex) where the higher functions belong. The inside of the brain is just as complicated and has many different parts, such as the hypothalamus that is involved in homeostasis, and the hippocampus that converts short-term memories into long-term memories.
How does a lump of cells weighing around 1.5kg produce such wondrous abilities such as philosophical thought, deduction, emotions and calculation? The truth is that we still do not know how the brain functions exactly. However, we know that the brain is composed of a large number of neurons (nerve cells) – about 100 billion of them. These neurons connect to one another via a synapse, which is a gap between two nerve cells where neurotransmitters travel to and fro (allowing electrical impulses to jump from one neuron to another). Using these connections, neurons form an unbelievably intricate and complex network of electrical activity. Because one neuron can connect to many more others, the number of synapses is estimated to be around 100~1000 trillion – significantly more powerful compared to any computer in the world. The number of synapses directly correlates to intelligence and it seems intellectual activities such as reading a book increases the number of synapses in the brain. We have yet to understand exactly how the brain uses this incredible computational power to produce cognition and self-awareness.
(Video of neuronal activities in a zebrafish brain)
Because the brain uses electrical impulses for most of its functions, a common abnormality that is seen with the brain is when the electrical activity becomes disorganised and out of control – a seizure. This abnormal electrical activity may be due to a focal problem such as a tumour, or a generalised misfiring of neurons or altered regulation of electrical activity. When a seizure happens, the disorganised activity results in the brain not being able to function normally. For example, the most common consequence is a fit (tonic-clonic seizure) where every muscle spasms out of control, because the muscles are overloaded with chaotic signals. Focal seizures can cause fascinating symptoms depending on the location, such as temporal lobe seizures causing religious visions (hallucination). This also disrupts consciousness, which is why most epilepsy patients do not remember the event.
On September 13, 1848, a 25-year-old foreman named Phineas P. Gage was working on a railroad with his work team. In an unfortunate turn of events, as he was using a tamping iron (large iron rod with a pointed end, measuring 3 feet 7 inches in length and 1.25 inches in diameter) to pack gunpowder into a hole, the powder detonated. The forceful explosion drove the metal pole skyward through Gage’s left cheek, ripped into his brain and exited through his skull, landing dozens of metres away. His workmates rushed to Gage’s assistance (who they presumed to be dead at the time of the accident), and to their surprise, found that he was still alive.
In fact, Phineas Gage spoke within a few minutes of the incident, walked without assistance and returned to his lodging in town without much difficulty – albeit with two gaping holes in his head, oozing blood and brain everywhere. He was immediately seen by a physician who remarked at his survival. In fact, it is reported that he was well enough to say: “Here is business enough for you” to the doctor. Another physician named Dr John Harlow took over the case, tended to the wound, fixed up the hole and recorded that he had no immediate neurological, cognitive or life-threatening symptoms.
By November, he was stable and strong enough to return to his home, along with the rod that nearly killed him. His family and friends welcomed him back and did not notice anything other than the scar left by the rod and the fact that his left eye was closed. But this was when things started to get interesting.
Over the following few months, Gage’s friends found him “no longer Gage”, stating that he was behaving very differently to the man who he was before the accident. Dr Harlow wrote that the balance between his “intellectual faculties and animal propensities” had seemingly been destroyed. Gage became more aggressive, inattentive, unable to keep a job, verbally abusive and sexually disinhibited. He would frequently swear using the most offensive profanities and would be as sexually suggestive as a March hare. How did the iron rod cause such a dramatic change in Gage’s personality?
Phineas Gage would go on to be one of the most famous patient case histories in the history of modern medicine. His case was the first to suggest some sort of link between the brain and personalities. Neurologists noted that the trauma and subsequent infection destroyed much of Gage’s left frontal lobe – the part of the brain that we now attribute to a person’s logical thinking, personality and executive functions. It is in essence the “seat of the mind”. Ergo, Gage’s loss of one of his frontal lobes meant that his control of bodily functions, movement and other important brain functions like memory were undisturbed, while his “higher thinking” was essentially destroyed (he was essentially lobotomised). This explains Dr Harlow’s observation of his “animal propensities”.
Thanks to this case, a great discussion was sparked and the idea that different parts of the brain govern different aspects of the mind was conceived. We are now able to localise almost exactly where the language area is, what part controls movement and how a certain piece of the brain converts short-term memory into long-term memory.
They say that human imagination is infinite and limitless. But consider this: can you imagine a colour outside of the visible spectrum? Most likely, you are incapable of thinking of a new colour that cannot be mapped on a standard colour chart. Interestingly, a small proportion of people can see and understand colours beyond the range that the majority of us can see.
The physiology of vision is rather complex, but essentially boils down to the retina (inside lining of the eyeball) acting as a film for the image that you see. Cells known as photoreceptors convert the visual image into electrical signals that are transmitted to the occipital lobe of the brain via the optic nerve. There are two types of photoreceptors: rod cells, which sense movement, and cone cells, which sense colour and provide sharp images (visual acuity). Human beings typically see colour by combining three primary colours: red, green and blue (known as the RGB system). There are cone cells for each primary colour. The brain processes the signals sent by each cone cells and figures out what “colour” you are seeing. Therefore, you can only perceive colours made from a combination of red, green and blue. It is easy to visualise this by playing with colour palettes on computer programs such as Photoshop.
In recent years, it has been speculated that a certain percentage of women have an extra type of cone cell that senses a different wavelength of light. Ergo, they can theoretically sense a greater range of colours compared to someone who has three types of cone cells. This condition is called tetrachromacy(“four colours”). Tetrachromacy is the opposite to colour blindness, which is caused by a deficiency or fault in one or two types of cone cells. To these people, the average person (a trichromat) will appear “colour blind”.
According to one estimate, as many as 12% of women are tetrachromats. Although there are many theoretical barriers to true tetrachromacy, there have been several documented cases of women who perceive colour in much more depth.
The ability to see an extra primary colour is more significant than just a 25% increase in the person’s colour range. An average person can see about 1 million different hues (shades of colours), while a true tetrachromat can see 100 million hues – a hundred-fold increase in the range of colours they can see. One can only wonder what kind of amazing sights a tetrachromat sees when she gazes upon a field of flowers or even a rainbow. Unfortunately, even if a tetrachromat tried to explain the colours she saw to us, we would not be able to grasp the colours as our minds would be incapable of visualising the colours, much like how describing the colour red to a blind person is impossible.
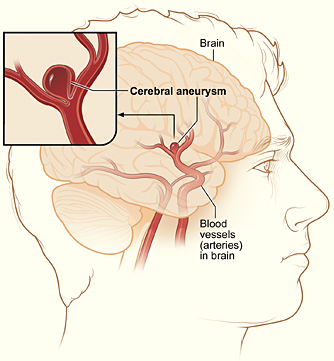
Stroke is a disease often associated with the elderly, but this is not necessarily true. As much as 5% of the population carry a ticking time bomb in their brain, known as a berry aneurysm. An aneurysm is a weakening of the arterial wall, causing a localised ballooning of the vessel. A berry aneurysm is a common type of aneurysm where the ballooning resembles a berry. What is most troubling is that a large proportion of these aneurysms can present very early (usually congenital, meaning you are born with it), with one research suggesting that 1.3% of the population in the age group of 20 to 39 has a berry aneurysm. If this berry aneurysm was to burst, no matter how young and fit you are, you will bleed into the area around your brain (subarachnoid haemorrhage), suddenly develop a severe, crippling headache (“thunderclap headache”), become confused, show signs of stroke such as speech or movement problems, or simply drop dead.
Fortunately, only 10% of people carrying a berry aneurysm suffer a ruptured aneurysm and subsequent brain bleed. The other 90% will carry on living their lives, without ever knowing that they had a time bomb in their brain.
Certain factors make the risk of the aneurysm bursting go up, such as high blood pressure, which can be caused by a stressful lifestyle or smoking. But in some cases, as explained above, even a healthy teenager could suddenly drop to the ground with a massive brain haemorrhage.
Berry aneurysms are only one of many ways death could strike unnoticed, no matter how young you may be. You could live a long and healthy life and die peacefully in your sleep when you are 90 years old, or you may have a stroke and drop dead in a few minutes’ time. For all you know, a bus might run you over tomorrow, with no warning whatsoever. Ergo, youth is not an excuse to waste the day you are given. You do not have to achieve something great, or be productive, but at least spend your day knowing that you are doing everything in your power to make yourself happy, without harming your health, your future or other people.
Consider this: if you see something that is not there, or not see something correctly, is that due to a problem in your eyes or your brain? An interesting anatomical fact is that the eyes are part of the brain. They originally evolved from the brain and drifted further and further forwards, connected to the brain by the optic nerves. If you lift a brain out from the skull, the eyes would be pulled backwards too. But technically speaking, eyes are distinct organs by themselves that have merely originated from a portion of the brain. It does not think or make decisions by itself. Just like a camera, an eye records things as it sees it and transmits it to the brain via the optic nerve via electrical signals. The brain then processes the signals in the occipital lobe, located at the back of the head (this is why you “see stars” when you bang the back of your head).
This means that vision can be altered anywhere along the pathway. If you have cataracts, where the lens of the eye becomes clouded, you lose portions of your visual field. If you have a large pituitary gland tumour, it presses on the optic nerve and causes double vision (diplopia) or vision loss. If you have a stroke in the occipital lobe, you can lose your vision. The brain’s role in producing vision can easily be demonstrated in the form of optical illusions. The eye merely records and transmits what it sees, but the brain becomes confused by what information it receives and tries to make sense of it. In the process, we experience bizarre illusions such as static images moving by themselves.
Because of this intricate pathway, some pathologies present with fascinating symptoms. A condition called Anton’s blindness (or Anton-Babinski syndrome) causes a patient to “see” despite being blind. Patients with Anton’s blindness are adamant that they can see perfectly clearly, and will even describe what they are seeing. However, what they “see” is completely different to what the object actually looks like. For example, if the patient looked at a blonde woman wearing a yellow blouse and a red skirt, they may describe her as a brunette woman wearing a blue shirt and black jeans.
The reason for their blindness is that their occipital lobe was damaged (usually by a stroke), leading to an inability to process the information from the eyes. Although the eyes are pristine and record what they see in perfect detail, the brain is incapable of interpreting the signals. The brain then goes on to confabulate, where the brain fills the gap by conjuring up false information. This makes Anton’s blindness quite hard to pick up on as the patient will not complain of it. It is only found when someone pays close attention to the patient and notices subtle cues like the patient bumping into furniture or talking in the direction where they think a person is at (even after they move). Ergo, the patient adamantly believes that they can see as their brain thinks it is seeing things (even though it is not receiving the information from the eyes properly).
Seeing is not believing. You see what you believe.
During the 1950’s when the field of neuroscience was making many research breakthroughs, a fascinating fact was discovered. Scientists had located the specific part of the brain responsible for feeling pleasure. In 1954, two Canadian neuroscientists named James Olds and Peter Milner were undertaking research to find the association between electrical stimulation of the brain and sensation in rodents. During their research, they found that if they stimulated a certain part of the brain, the rats would interpret the signal as pleasure. Based on this, they inserted electrodes into the rats’ limbic system (the part responsible for emotions) and connected it to a lever in the cage. Thus, they had devised a device that allowed the rat to feel pleasure by stimulating its own brain with the press of a lever. The results were astounding. The rat furiously pumped at the lever, forgetting to eat or sleep, until it ultimately died of exhaustion (over 26 hours, the rat pressed the lever 50,000 times).
Pleasure is not the same as happiness. Happiness awards us with satisfaction and contentment, but pleasure only brings greed, obsession and addiction. Pleasure was originally a mechanism devised to reward behaviour that aided survival (such as mating and eating), but addictive things like alcohol, smoking and drugs ruin your life and any chance at happiness instead of helping you survive.
The foolish run around to seek temporary pleasure while the wise seek permanent happiness.
Occasionally, there are news stories about a man who eats steel or a girl who likes to eat plastic. Such a condition where the person develops an appetite for a non-food substance is called pica. Pica is more common than one would think. The most common cases are those of dirt, clay and chalk, with the disorder being much more prevalent in children or pregnant women. Although pica is officially a mental disorder (possibly related to OCD), it is possible that it is a neurological mechanism to cure a certain mineral deficiency. For example, patients with coeliac diseases or hookworm infections tend to be iron-deficient and the substances they eat tend to contain iron. It is unclear how the brain knows what “food” to eat to cure a disease, but there are many cases where people subconsciously consume foods that would improve their health. According to a study, between 8% and 65% of people have had a sudden urge for a very strange appetite. However, as substances commonly involved in pica (such as dirt and ice) are solids, they can damage the oesophagus and the digestive tract. Also, they may contain toxic chemicals which can cause poisonings, making pica a potentially dangerous condition.
What exactly is the present? The present is the middle point between the past and future, the world that we experience and perceive on a real-time basis. But would you believe it if the world you perceive is not the true “present”? To experience the world, we use our five senses. The brain collates all these sensory information and processes it to construct “the present”. This process takes about 80 milliseconds. Ergo, the world we experience is actually the world as it was 80 milliseconds ago. For a similar phenomenon, consider the stars. The stars we observe are not what they look like now, but what the stars looked liked when they emitted the light that we see. Thus, the star you are looking at may not even exist anymore.
But 80 milliseconds is a very short time; surely it has no impact on our everyday life? To prove that this delay has a critical impact on our understanding of cause and effect, neuroscientists designed the following experiment. The researchers would ask the participant to press a button that caused a light to blink after a short delay. After about ten tries, the participants reported that the delay had disappeared and the light flashed immediately after they pressed the button. This was due to their brain editing out the time delay and directly connecting the cause (button) and the effect (flash). But a much more peculiar phenomenon was seen when the researches removed the delay between the button press and the flash. Participants reported that they saw the light flash before they even pressed the button. The participant’s brain had become so used to the editing process that it was confusing the order of the cause and the effect.
The brain’s time-editing ability can be seen in the following simple experiment. If you touch your nose and toe at the same time, logic dictates that as the toe is further from your brain, the signal will have to travel further and it will be felt later. But in reality, you feel both at the exact same time. This is because your brain uses a map of the body to edit the relative time the signal takes to reach the brain to better construct a “real-time present”.
A person’s body temperature is always maintained between 36.5~37.5°C. This is because enzymes, which are crucial in all physiological reactions in the body, work most efficiently at this temperature. As physiology is essentially a series of chemical reactions, it is heavily dependent on temperature. If the temperature falls, chemical reactions occur slower and vice versa. When body temperature falls below 35°C, metabolism becomes too slow and it poses a risk to the person’s health. This is known as hypothermia.
How does hypothermia affect the body? Hypothermia is categorised into three classes depending on the severity.
Mild hypothermia (32~35°C) leads to the slowing of bodily functions, tremors and difficulty in walking. The patient’s speech is impeded and other neurological symptoms such as decreased judgement skills and confusion start to appear. Also, blood pressure, pulse and breathing rate rise.
Moderate hypothermia (28~32°C) causes paralysis of muscles and extreme fatigue (they may complain of being sleepy). As blood (carrying heat) is rerouted to major organs, the skin (especially lips and extremities) become white or purple and very cold. Neurological symptoms worsen with amnesia, memory loss, severe confusion and delusion beginning to show. As sustained hypothermia leads to the tremors stopping, one should not take the lack of tremors as a good sign. Heart rate becomes irregular and arrhythmia may occur.
Severe hypothermia (20~28°C) leads to chemical reactions becoming so slowed that physiological functions that support life decline dramatically. Heart rate, blood pressure and breathing all lower to dangerous levels and the heart and lungs may stop functioning. As the patient’s major organs begin to shut down, they enter a state of unconsciousness and eventually, clinical death.
As you can see, hypothermia is a highly dangerous situation that can kill. There are some other fascinating facts about hypothermia.
20~50% of hypothermia death cases are associated with paradoxical undressing. This is a strange phenomenon where the person begins to take off their clothes due to confusion and a lack of judgement from the hypothermia. One theory suggests it is related to the cold damaging the hypothalamus (which controls body temperature), causing the brain to think that the body temperature is rising. Whatever the reason, it is extremely dangerous as it worsens the hypothermia.
As explained above, severe hypothermia leads to death. But interestingly, hypothermia also protects organs. This is why organs for transplanting are transported in ice. Similarly, there are examples of people who “died” from hypothermia recovering with no brain damage. Because of this, medical professionals traditionally say: “they’re not dead until they’re warm and dead”. In fact, if there is something wrong with the patient’s circulation and there is risk of damage to their organs (such as in surgery), sometimes the patient’s body temperature is forced down with ice water injections and cooling blankets, known as protective hypothermia.